

Welcome to the Scrambler Therapy® official scientific and clinical information site
Welcome to the Scrambler Therapy® official scientific and clinical information site
Electro-analgesia was first introduced in an empirical form, utilizing at first animal sources of electricity (torpedoes), then static, galvanic and alternate sources, to the most modern TENS and implant devices. The Electro-analgesia theoretical reference basis was created by R. Melzack and P.D. Wall, who in 1965 published the Gate Control theory ( Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 150(699):971-9, 1965 ).
 This theory is still today a primary theoretical reference for all electro-analgesia and neuro-modulation procedures, even if it is not considered exhaustive. On the other hand, both technological and implant stimuli techniques have greatly changed over time. In general, the ultimate purpose of these techniques is always to inhibit pain impulse transmission using an electric stimulus (of various nature depending on the device utilized). In scientific literature there are reference works that define limits and application fields of the various techniques and technologies used today, to be consulted for further information on this issue.
This theory is still today a primary theoretical reference for all electro-analgesia and neuro-modulation procedures, even if it is not considered exhaustive. On the other hand, both technological and implant stimuli techniques have greatly changed over time. In general, the ultimate purpose of these techniques is always to inhibit pain impulse transmission using an electric stimulus (of various nature depending on the device utilized). In scientific literature there are reference works that define limits and application fields of the various techniques and technologies used today, to be consulted for further information on this issue.
The Gate Control theory, though widely applied in the historical development of electro-analgesia, has significant limitations concerning the analytical representation of chronic pain in its various neurological and pathological mechanisms. The most significant observed gap is that while this theory can interpret "mechanical" pain transmission methods, it cannot interpret properties of the associated information, such as emerging properties and pain response in the most elevated and complex systems such as memory and learning. These responses are non-linear and dynamically variable through time, compared to the pain stimulus itself.
Even though the CNS by nature continuously generates and processes data, this is never explained analytically and theoretically, only in very generic descriptive terms such as "electrical impulses", therefore missing a fundamental characteristic description. This limitation of the theoretical analysis is not a problem for devices that work on the inhibition of pain transmission, since their implicit purpose is to suppress this information. This analysis is relevant however in the different type of approach for the theoretical and analytical study of pain control that led to the creation of the Scrambler Therapy.
Therefore, considering these facts, in order to exceed efficacy limits of protocol cures, a different reference model has been developed. Basically, it was necessary to create a more appropriate theoretical model to cybernetically interpret the dynamics of the pain system (processes of communication and regularization) and the system's complexity in order to explain the non-linear and complex dynamics of chronic pain. The developed theoretical model analyses the immediate effects (instant analgesia during treatment) and the medium/long term remodeling (thresholds) of the pain system as far as perception is concerned.
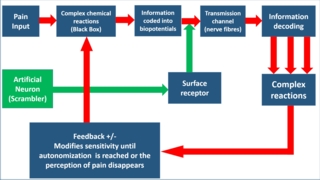 In order to achieve this goal, it was necessary to implement the information theory in a more complex analysis system, based upon a "black box" in which the complexity level of emerging properties that characterize pain information was fixed arbitrarily on the genesis of action potentials that trigger a chain of pain information transmission. This modality implicitly includes the role of the various molecules involved in the modulation of pain (all virtually included in the black box), as they are functionally represented by involved action potentials.Therefore, this model no longer treats action potentials as simple "impulses," but as complex information strings.
In order to achieve this goal, it was necessary to implement the information theory in a more complex analysis system, based upon a "black box" in which the complexity level of emerging properties that characterize pain information was fixed arbitrarily on the genesis of action potentials that trigger a chain of pain information transmission. This modality implicitly includes the role of the various molecules involved in the modulation of pain (all virtually included in the black box), as they are functionally represented by involved action potentials.Therefore, this model no longer treats action potentials as simple "impulses," but as complex information strings.
It may thus be reasonably assumed that it is possible to control the lower levels of the complexity of the pain system (the chemical reactions regulating the coding of pain information and subsequent feedback) by manipulating the "information" variable alone at higher levels of complexity.
To further comprehend the information concept utilized see the information theory (Claude Shannon, 1948). In a nutshell, information requires a coding system based on signs and rules. For example, the alphabet expresses signals, but rules are necessary in order to create meaningful sentences for the reader.
Letters assembled in a random manner, although recognizable as signals, do not constitute information. Similarly, action potentials generated sequentially by a stimulated receptor cannot be interpretable without an analytical model of "information coding" rules. For example, frequency modulation of action potentials gives us an idea of the stimulus intensity, but it does not tell us how its perception is coded in terms of different sensations, nor does it tell us how thermal sensation is coded differently from painful sensation with respect to information. Actually, based on simple coding of information in frequency modulation, it would theoretically and technically be possible to artificially reproduce any kind of sensation, but we know this is not so. This problem of coding/decoding system analysis in the C.N.S. does not limit itself only to frequency modulation. If this were true, any type of sensory trick could have achieved it using very simple technologies.
During the development of Scrambler Therapy, artificial neurons were developed to transmit to the C.N.S. information recognizable as "self" and "non pain" in a non-invasive manner through surface C receptors. Compared to the conventional electro-analgesia, the assumed active principle that is currently under trial is not to inhibit pain transmission (through A-beta fiber excitation), but to substitute pain information with synthetic "non pain" information.
The study’s main focus is to continue the theory validation process through always more meaningful progressive testing proof, clearly consistent with the developed method’s expectations and emerging data. In this case, considering this theory model’s expected high analgesic efficacy in cases not normally responsive or poorly responsive to the most effective drug protocol treatments, and conventional electro-analgesia (TENS, implanted devices), the normal reference testing model is a perspective comparative clinical study. The advantage of this approach is that it can also compare the study’s emerging results with a broad and diversified scientific literature. This enables comparisons with well-consolidated scientific data coming from different sources. Biochemical or image studies of clear interest .
All theory models need an experimental test that must produce outcomes in line with foreseen expectations. Until today, the published studies and clinical routine experience have confirmed the expectations of the ST theory model. More in-depth validation will be achieved through neuroimaging to better highlight related plasticity phenomena, and, from my point of view, from studies of central pain. In waiting for further validation by independent studies, some basic points have been relatively well established:
• Currently we are aware that C fiber excitation produced by ST is not compatible with the Gate Control theory. Electrical C fiber excitation without information (ie simple electrical impulses not encoded as "no pain information") should produce pain, whereas, in line with theoretical expectations, it rapidly produces analgesia.
• The broad scientific literature on the analgesic effect of placebo and hypnosis shows pain relief far lower than the ability of ST to markedly reduce pain during treatment.
• The effect of a treatment cycle is prolonged in time. Difference in time of a treatment carried out correctly depends on the stability of the neurological damage. If the neurological damage is stabilized, the treatment effect tends to be decisive. Differently, relapse tends to follow the time-lapse and intensity of the neurological damage progression.
• Different from other forms of electro-analgesia, resistance phenomena in cases of repeated treatments are unknown. Clinical experience partly published confirms that each new treatment cycle fully keeps its efficacy and overall calls for less treatments than the initial ones.
• Higher clinical efficacy is recorded in chronic persistent pain with meaningful neuropathic implications (present also with oncological pain), which typically is not responsive to other treatments. This aspect is consistent with the remodulation assumption of the pain system due to the effect of “non-pain” information. Similarly, in physiologic/acute pain, where plasticity is not meaningful, Scrambler Therapy behaves simply as a symptomatic therapy used when needed. This double-aspect in efficacy is also consistent with theory expectations.
• A final clue to ST’s hypothesized analgesic role is the rapidity with which analgesia occurs, and the difference in perception felt by the patient compared to other forms of electro-analgesia. To produce a total and immediate analgesic effect by ST, it is sufficient for the patient to feel a circumscribed stimulation below the area of the electrodes, which are of reduced dimensions (EKG single-use type). It is therefore not necessary to feel the stimulus in the pain area or areas of paraesthesia.
• Immediately after the treatment, no type of paraesthesia or anesthesia is recorded. The physiological response to evocated pain remains unchanged, notwithstanding the clear analgesic effects on chronic pain. This result tends to rule out a prolonged period of C fiber refractoriness, and plays in favor of the re-modulation of the pain system’s response carried out by synthetic information of “non-pain”, as assumed in the theory.
• In conventional electro-analgesia TENS systems currently known it is necessary to exclude C fiber stimulation, since electrical stimulations might provoke pain. This is the reason why conventional TENS, notwithstanding other stimulation features (frequency, intensity, modulation, burst) rarely provide maximum pulse width higher than 250 microseconds. The ability of Scrambler Therapy to constantly operate with impulses suited to stimulate C fibres offers confirmation that it is different from the Gate Control Therapy and from analgesia limits produced by conventional TENS.
Contact Download Video Tutorial Delta Research & Development
Copyright © Delta Research & Development. All rights reserved